The Reproductive Facts from The American Society for Reproductive Medicine
 A 37-year-old woman goes to her doctor for evaluation and treatment for infertility. She has never been able to get pregnant and very much wants to have a baby. She has bleeding for 10 days with her periods and she says she has feelings of fullness in her pelvis and pain during her period. Intercourse can be painful at times and she often battles constipation. During her physical examination, her doctor feels a large mass on her uterus and recommends further testing.
A 37-year-old woman goes to her doctor for evaluation and treatment for infertility. She has never been able to get pregnant and very much wants to have a baby. She has bleeding for 10 days with her periods and she says she has feelings of fullness in her pelvis and pain during her period. Intercourse can be painful at times and she often battles constipation. During her physical examination, her doctor feels a large mass on her uterus and recommends further testing.
An ultrasound shows a mass measuring 10 cm (about 4 inches) in diameter. The mass, which the doctor believes is a fibroid tumor, extends into the cavity of her uterus. Her doctor talks with her about several treatment options and she chooses to have a myomectomy. This procedure allows the tumor to be surgically removed from her uterus using a minimally-invasive technique. She recovers quite well and 3 months later, while completing some of the testing for infertility, she gets pregnant. She has no complications during her pregnancy and delivers a healthy girl at 9 months through a cesarean section.
Uterine Fibroids
This story is quite typical for many reproductive-aged women. Uterine fibroids are also called myomas or leiomyomas. These are benign tumors, meaning they are not cancerous. They are quite common and can affect between 30 and 50% of women of reproductive age. It is estimated that uterine fibroids will affect 8 in 10 African American women and 7 in 10 Caucasian women by menopause.
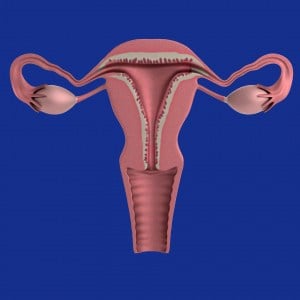
Let’s begin with some basic anatomy. The uterus is a muscular, hollow, pear-shaped organ that contains and nourishes the embryo and fetus from the time the fertilized egg is implanted to the time of birth of the fetus. It lies in the pelvic cavity between the bladder and the rectum. The nonpregnant uterus is approximately the size of a clenched fist.
There are two main parts of the uterus – the body and the cervix. The body has strong, muscular walls that expand during pregnancy. The cervix is the lower part of uterus that joins the vagina.
There are two main layers in the body of the uterus: the myometrium is the muscular wall forming the main mass of the uterus. The endometrium is the inner layer of the uterus that undergoes changes throughout the menstrual cycle.
Fibroids develop from genetic changes in a smooth muscle cell within the myometrium. The cell multiplies to form a tumor. The exact cause of uterine fibroids is unclear, but there is evidence that it may be a combination of both genetics and hormones.
Fibroid growth is regulated by many different factors, including hormones. Estrogen and progesterone (hormones produced primarily by the ovaries) may stimulate growth of the fibroids. And, after menopause, when hormone levels are low, fibroids rarely grow and frequently shrink. Maintaining a healthy diet and exercise seem to reduce the risk of fibroids. Medications such as low-dose birth control pills have little or no impact on fibroid growth.
Fibroids are usually found in or around the body of the uterus, but sometimes occur in the cervix. Fibroids within the uterus can be divided into three categories: subserous, located in the outer wall of the uterus; intramural, found in the muscular layers of the uterine wall; and submucous which can protrude into the uterine cavity (Figure 3). In addition, fibroids can be connected to the uterus through a stalk (called pedunculated). About 55% of fibroids are subserosal; 40% are intramural; 5% are submucosal. Fibroids are rarely found outside the pelvic cavity.
Symptoms from fibroids are related to their size and location. Although most women with fibroids have no symptoms, many may have significant symptoms, including pelvic and abdominal pressure or pain and excess bleeding. Approximately one-third of women with fibroids will have abnormal uterine bleeding, pain or pressure in the lower abdomen. Women with fibroids pushing into the cavity of the uterus often have irregular bleeding and may have problems with fertility. Fibroids in the muscle or just beneath the outer surface of the uterus are more likely to cause pressure, pain, and affect nearby organs, such as the bladder or rectum. This image shows a uterus with a large fibroid. Sometimes, fibroids can enlarge so much that they change the shape of the uterus.
Let’s discuss some of the common symptoms associated with fibroids.
Abnormal uterine bleeding is the most common symptom associated with fibroids and is the main reason women seek treatment. Intramural and submucosal fibroids can distort or enlarge the uterine cavity. Pressure from submucous fibroids on the endometrium can cause excessive bleeding. Because abnormal uterine bleeding can result from other causes, such as endometrial cancer and hormonal problems, it is important that women with fibroids who have abnormal vaginal bleeding receive a thorough evaluation for other causes of bleeding.
Pain is a common symptom of fibroids. Women with fibroids may have painful menstrual cramps.. A rapidly enlarging fibroid may outgrow its blood supply and degenerate, causing pain and cramping. Pedunculated fibroids, which are attached to the uterus by a thin stalk, may twist and cause severe pain. Large uterine fibroids, or those which push on the bowel, the vagina, or pelvic wall may also make bowel movements, sexual intercourse, or certain movements painful.
Large fibroids may press on nearby pelvic organs. If the fibroid presses on the bladder, which lies in front of the uterus, a woman may have urinary frequency or urgency as shown in the MRI image here. Pressure on the ureters, which are the tubes that transport urine from the kidneys to the bladder, can result in kidney damage if the fibroids are not removed. Fibroids in the lower uterus may put pressure on the large bowel and rectum, which could cause painful bowel movements, constipation, changes in the shape of stools, or hemorrhoids.
Fibroids may affect fertility and can impact pregnancy. Uterine fibroids are found in 5-10% of infertile women. However, fibroids are the single cause of infertility in only 2-3% of these women. So it’s important for infertile women and their partners to have a thorough investigation to identify other causes of infertility.
There are several explanations for why uterine fibroids may affect fertility:
- Changes in the position of the cervix (the vaginal opening to the womb) from the fibroids above may affect the number of sperm that can travel through the cervix.
- Changes in the shape of the uterus can interfere with sperm movement.
- Changes in the uterine muscle which prevents movement of the sperm or embryo.
- Inflammation in the wall of the uterine cavity which can affect implantation.
- Effects on the blood flow to the uterine cavity where the embryo would implant.
- Blockage of the fallopian tubes by the fibroids.
- The egg and tube are separated by fibroids and the egg cannot find its way into the tube.
If the fibroids are in the uterine cavity or push on the fallopian tubes, they can affect a woman’s fertility. However, it is not clear whether fibroids in the uterine muscle affect fertility if they do not directly influence the movement of sperm, egg, or embryo. In a study of women with unexplained infertility, the chance of pregnancy was 25% for a woman who did not have fibroids. For women with fibroids, the chance to get pregnant was 11%. In women who had fibroids but had them removed, their chance to conceive was 42%. This shows that fibroids may play a role in hampering a couple’s ability to conceive.